Peritonsillar abscess (PTA) is a common infection of the peritonsillar space usually caused by mixed aerobic and anaerobic flora. PTA can occur de novo or with a preceding recent history of tonsillitis. The abscess usually involves the loose connective tissue between the capsule of the palatine tonsil and the pharyngeal muscles.
A common location for abscess formation is seen superior to the tonsil and involves the soft palate, often without crossing midline. Another less common theory of pathophysiology of PTA involves the Weber glands, salivary glands found superior to the tonsils, that can become blocked either by simple debris or via scarring and fibrosis of the ducts secondary to infection of the tonsils and soft palate. Blocked Weber's glands can then lead to abscess formation.
Common infecting organisms include Streptococcus pyogenes (30%), H. flu, Staph aureus, Streptococcus viridans, Streptococcus sanguis, and Fusobacterium. As stated previously, 90% of cases are mixed aerobic and anaerobic infections with multiple infectious species and warrant broad spectrum antibiotic therapy.
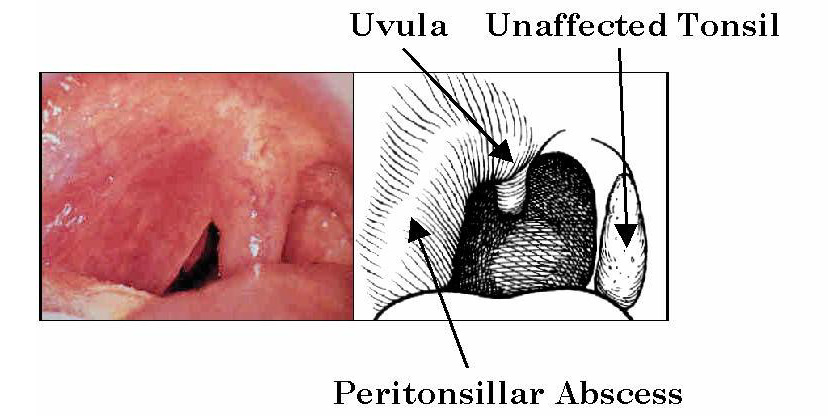
45,000 cases of PTA are reported annually with a broad patient base involving all ages and genders. The highest incidence occurs in those 30-50 years of age. Patients most commonly present with a 3-5 day history of sore throat, headache, dysphagia, vocal changes, difficulty opening mouth, neck pain, and referred pain to the ear. On physical exam these patients are found to have edema and swelling of the oropharynx superior and lateral to the tonsil. The tonsil may be visibly erythematous, enlarged, or covered with exudate. The uvula is often deviated away from the affected side. Trismus is a common exam finding and is associated with swelling and inflammation of the internal pterygoid muscles. Other possible findings include fever, halitosis, and lymphadenopathy on affected side.
Differential
The differential diagnosis for PTA includes peritonsilar cellulitis, pharyngitis, epiglottitis, dental infections, and mononucleosis. Less common diagnoses to keep in the back of your mind include: tumors, carotid aneurysm (not a great place to stick a needle), tracheitis, and Ludwig angina (submandibular/sublingual space infection). These differential diagnoses are clearly delineated from PTA through a precise workup including:
1) CBC with differential to isolate the presence of a bacterial infection.
2) Imaging: Intraoral ultrasound has clearly become the imaging modality of choice for the diagnosis of PTAs. US provides a quick, cheap, and accurate means for determining the presence, size, and anatomic location of an oropharyngeal abscess. Additionally, US provides a means of determining the relationship of the PTA to the carotid artery - a crucial factor sould drainage be desired.
3) CT is an alternative to US in such instances when the patient is unable to open their mouth due to trismus.
Treatment
Once the diagnosis of PTA has been confirmed using US or CT, treatment can be initiated. The patient should first receive adequate analgesia and hydration due to the risk for severe dehydration in PTA. A clinical decision is then required to determine the need for needle aspiration of the abscess or surgical incision and drainage. For cases in which the patient has no deep tissue invasion, sepsis, or toxicity, the abscess can be drained in the ED using perimucosal needle aspiration. However, if the PTA is complicated by invasion of the deep neck tissues, close proximity to the internal carotid, or by poor patient cooperation, a otolaryngology consult is justified.
Needle Aspiration
Perimucosal needle aspiration should be performed after ultrasound confirmation of the abscess and location of the internal carotid in relation to the abscess. The depth of the PTA and the internal carotid can be measured using the US machine and used to tailor the aspiration procedure. The needle guard should be removed from the needle and cut to a length such that when placed back on the needle, sufficient needle is exposed to pierce the mucosa and reach the abscess but not puncture the internal carotid. For example, if a PTA is found to be 1.5 cm deep in the soft palate, cutting 1.5-1.75 cm off the needle guard should be sufficient to reach the abscess without endangering the carotid. Needle aspiration of PTAs typically produces 1-20cc of purulent material from the abscess. Success of the procedure can be determined with a second intraoral ultrasound which should show a reduction of the abscess. Alternatively, the procedure can be viewed in real time using ultrasound guided aspiration and the abscess can be visually reduced. This modality is of great benefit when the abscess is loculated or more complex.
Antibiotic therapy must cover gram(+) intraoral flora and anaerobes. The commonly accepted treatment for PTA includes Flagyl in combination with penicillin (erythromycin in penicillin allergic patients). Combination found to be curative in 98% of patients.
References: